Lived Experience workers are ‘change agents’ providing a resource to support personal change for service users and cultural and practice change in the service. This dual focus is a unique characteristic that requires other health professionals and employing organisations to actively partner with the Lived Experience workforce. Understanding the dual focus is the first step towards workforce development.
A resource for change
Lived Experience workers provide a resource for change: the personal and social change that provides the necessary foundation for individual recovery, and the cultural and practice change that can move health care services towards recovery-oriented practice.
The relationships made possible through Lived Experience work strengthen connection, resiliency, choice, and hope, improving the lives of individuals and assisting to transform services.
Positive relationships are the starting place and necessary foundation for connection between service users and service providers. They are also an essential element in helping people to build recovery resiliency, reducing the negative impact of future experiences of illness. Relationships also play a key role in enabling workplace change. Engaging individual practitioners is the critical point at which change becomes embedded in practice. Developing trusting relationships takes time, and the experience and credibility which is found in Lived Experience work. The following table illustrates the connection between the relational work of the Lived Experience workforce.
Table 1: A model of Lived Experience roles
| Change mechanisms (1) | Change mechanisms (2) | Process outcomes | Impacts |
|---|
- • Building trusting relationships based on Lived Experience.
- • Establishing a connection.
- • Enabling talking and listening.
| Role-modelling recovery and living well with mental illness | Personal outcomes - • hope
- • empowerment
- • social functioning
- • self-care
| Personal recovery and wellbeing |
| | Bridging between mental health professionals and service users | Engagement between service providers and service users | Service use - • improved clinical outcomes
- • reduced acute and crisis-care
|
| | Developing mental health professional understanding of recovery | Recovery-oriented workplace culture and practices | Effective services demonstrate return on investment |
(Based on a model by Gillard, Gibson, Holley and Lucock, 2015)
Benefits of the Lived Experience workforce
A well supported Lived Experience workforce results in benefits for people accessing services, families, social networks, and organisations, as well as the broader community.
Benefits that can be measured within the individual service setting include:
- improved rates of engagement and retention in treatment.
- reduced critical incidents or need for restrictive practices.
- improved self-management.
- reduced need for readmission or acute care.
- improved staff retention, safety and wellbeing.
Benefits for all
- Social justice
- Equality
- Diversity
- Increased value of lived experience
- Greater wellbeing and inclusion
- Improved culture for safe sharing
- Challenge discrimination and prejudice
- Increased hope and optimism – raising expectations of what is possible for people with lived experience
Benefits for families, carers and social networks
- Lived understanding aids rapport and relationships built on connection and trust
- More equitable relationships
- Foster a sense of belonging/community
- Focus on human rights/social justice
- Living example of hope
- Increased empathy
- Advocacy
- Mutuality
Benefits for people accessing services
- Risk adverse approaches replaced by dignity of risk
- Lived understanding aids rapport and relationships built on connection and trust
- More equitable relationships
- Foster a sense of belonging/community
- Focus on human rights/social justice
- Living example of hope
- Increased empathy
- Advocacy
- Mutuality
Benefits for organisations and colleagues
- Greater recovery understanding/orientation
- Contribute to more person-directed approaches
- Co-production leads to safer and more accountable services
- Contribute to more inclusive, flexible, resilient work culture
- ‘Bridge’ of understanding between people accessing services and colleagues in traditional roles
- Reduced need for ongoing formal support and hospitalisation
What informs Lived Experience work?
Lived Experience workers bring a ‘whole of life’understanding to the complex circumstances each service user is trying to navigate. Lived Experience workers are boundary spanners able to work between individual, community and service provider, bridging the gulf of service engagement. An effective Lived Experience workforce is recruited to reflect and engage with the diverse experiences of service users and the local community.
Lived Experience work is not only informed by a person’s individual experiences but also universal experiences of discrimination, marginalisation, exclusion and feeling powerless. In the case of personal Lived Experience roles, common experiences also include loss of identity/human rights/citizenship. Importantly, people in Lived Experience roles have experienced loss of hope and understand that regaining hope is essential.
Originating alongside other human rights movements, the concepts and practices of the consumer movement have grown in sophistication. Collective lived experience views enable people to reframe their own lived experience in ways that are healthier and more helpful, as part of a whole life, rather than the defining or limiting characteristic.
Accessing services, particularly involuntarily, includes surrendering a degree of control and autonomy. Returning to self-agency can be a long and difficult process and is not something people are taught how to do. As a result, at times people who access services can develop what is known as a ‘patient identity’, taking a more passive role in decisions, becoming overly dependent on the opinions of others. There is also a risk of self-stigma: learning to view oneself as fundamentally flawed or ‘less than’ other people. Particularly for people in personal lived experience roles, part of the work involves regaining a stronger sense of self by challenging unhelpful and damaging messages or beliefs and creating a new identity based on ideas that empower and build hope.
All Lived Experience workers share a humanistic focus, with relationships as central to the work. By virtue of the common experiences shared by Lived Experience workers and people accessing services, these relationships can work towards being more equitable and with a lesser power imbalance than traditional service provider/service user relationships.
Lived Experience work is based on common experiences, some of which can be traumatic or draining for workers to remember and engage with. Employers need to consider this emotional cost in work planning and allocate time for processing, debriefing and ensuring access to Lived Experience supervision and networks.
The uniqueness of Lived Experience roles
The starting point for understanding the uniqueness of Lived Experience work is the recognition of its specialist knowledge and experience base.
Unique knowledge, abilities and attributes
- Profound life-changing mental health challenges that have led to a new life direction and concept of self or life-changing experiences while supporting someone with mental health challenges that have profoundly impacted their life/world view.
- Personal identification with, and experiences of service use and/or advocating for someone using services.
- Understanding experiences of marginalisation, exclusion, discrimination, loss of identity/human rights/citizenship.
- Willingness to purposefully share experiences and parts of personal story in work role.
- Understanding both experiences of hopelessness and the critical need for hope – how to move from a position of hopelessness to one of hope.
- Willingness to use emotional understanding and knowing as key to work role.
- Willingness to be vulnerable and publicly ‘out’.
- Understanding the personal impact of experiences of trauma.
- The degree of empathy and what they are able to understand and empathise with.
- Greater equality and efforts to reduce power imbalances with people accessing services, including no involvement with coercive or restrictive practice of any kind.
- Being an advocate/change agent.
- Level of awareness about self-care and skills/strategies to prioritise it.
What makes Lived Experience work effective?
- Applying lived expertise: not just having a lived/living experience but what has been learned through that experience and how it’s applied.
- Links with and understanding of the wider consumer movement and concepts.
- Work that is values-based and authentically lived experience-informed, person-directed and aligned with recovery principles.
- A social justice and fairness focus informed by understanding power imbalances.
- Significant understanding and ability to use personal story effectively and appropriately, for the benefit of the other person or system/service reform.
- Convey or inspire optimism and hope.
- A bridge between organisations and people accessing services/supporting people accessing services.
- Understanding of overlapping identities and experiences (intersectionality) and the impacts of culture and identification.
- Trauma-informed: awareness of the role/impact of trauma and how to respond sensitively and appropriately.
- Resilience in the face of discriminating, prejudicial and disempowering attitudes, practices and policies.
- Focus on the relationship.
- Greater flexibility/scope/ability to be responsive to the person, rather than being driven by a prescribed agenda.
- Specialisation may be useful depending on the context and experience e.g. people from the Deaf community, Youth, people with experiences of family violence etc.
Values and principles informing Lived Experience work
Lived Experience roles, regardless of position type or level of authority, are distinguished by a commitment to using lived experience to benefit others, uphold human rights and achieve systems transformation. Lived Experience workers frequently talk about having personal investment in the work and the desire to help improve mental health systems and build a more inclusive society. Lived Experience workers identify as change agents: actively contributing to ongoing transformation of service design and delivery. This may take on an added layer of responsibility and drive for change for Lived Experience workers in representative roles from diverse cultures and communities including: Aboriginal and Torres Strait Islander, culturally and linguistically diverse and LGBTQIA+ communities.
Values at the heart of Lived Experience work
Lived Experience work is values-based, with values acknowledged as important in setting priorities in Lived Experience practice. For Lived Experience workers, practice that matches values leads to job satisfaction, whereas a mismatch of values and practice is a source of tension.
Embedding Lived Experience work involves embracing difference, accepting that different perspectives can be equally valid and important, and respectfully renegotiating influence and approaches to shared decision-making. Peer to peer work is based on principles of reciprocity and equality, each person giving from their experience for mutual benefit. When Lived Experience workers engage with other health professionals, they need a similar respectful exchange of knowledge as they mutually contribute to problem solving. Lived Experience workers need to experience equity, fair and impartial inclusion. This type of equality is a fundamental aspect of human rights.
Ultimately, Lived Experience work is distinguished not so much by what Lived Experience workers do but how they do it. The how is guided by Lived Experience work principles and values. Values are the pillars of the Lived Experience workforce and inform Lived Experience practice. The following lists of values and principles have been developed from reviewing existing literature and engagement with the Australian Lived Experience workforce.
Regardless of the role and position, Lived Experience work focuses on how lived experience is collectively understood and applied to benefit others, and used to contribute to system change.
Importantly, organisational support enhances the efficacy of Lived Experience work allowing this potential for contributing to system change and advocacy to be realised.
Table 2: Core values of Lived Experience work
| Core values | What does it mean? |
|---|
| Hope | Belief in people’s fundamental capacity to overcome challenges |
| Equality/equity | Working from a place of common humanity and vulnerability.
Actively working to minimise power imbalances. |
| Mutuality | Being in a relationship with another person where both people learn, grow and are challenged through the relationship. Sharing responsibility in relationships. |
| Empathy | Understanding another’s experience from a point of common experience and genuine connection. |
| Choice | Acknowledging and respecting each person’s choices, dignity of risk and boundaries.
Acknowledging that the person is the expert of their own experience. |
| Respect | Honouring another’s view and experience without judgement or making assumptions. |
| Authenticity | Integrity, being open, honest, trustworthy, and transparent in work practices and relationships.
Valuing the use of lived experience and vulnerability in the service of others transforms these from what may have been perceived as weaknesses into strengths. |
| Belonging/inclusion | Respecting and understanding the value of inclusion and impact of exclusion.
Recognising intersectionality and valuing diversity culture, spirituality, membership in chosen groups and community. |
| Interdependence/interconnectedness | Recognition that we exist in relationships and that the relationships with families and/or social networks are often impactful in our lives and important to healing. |
| Justice/Human Rights | Understanding the impact of social justice/inequity on identity and opportunity e.g. race, culture, sexual orientation. Recognising that equal access to resources and support is an important factor in everyone’s recovery and healing. Recognising the consumer movement as a response to the history of social injustice and discrimination towards people with lived experience. Recognising how Lived Experience work is connected to the human rights movement and upholding the human rights of people with lived experience. |
Guiding principles
Guiding principles flow from values, and shape how Lived Experience work is practiced. In essence, principles embody the ‘character’ and philosophy of Lived Experience workforce. These principles are written from the perspective of the Lived Experience workforce. However, principles inform practice and are also intended to guide and inform funding bodies/policy makers and organisations in developing Lived Experience roles, designing programs, and deciding policy.
Table 3: Guiding principles
| Principles | What does it mean? |
|---|
| Lived Experience as expertise | The expertise that arises from a lived experience is of equal value to other types of expertise, including academic qualifications. |
| Self-determination | Respecting individual choice and personal agency. |
| Recovery-focused | Recognises that individuals can define what recovery/healing means to them, and each person can create a life that is meaningful for them. Interactions are underpinned by hope. |
| Person-directed | Service access and individual recovery planning/journey is directed by the person themselves and recognises the person as the expert of their own experiences. Respects where each individual happens to be in their journey of recovery/healing, and recognises that goals, values, spirituality, beliefs, and choices will be unique to each person. |
| Strengths-based | Identifying and drawing on existing strengths to support growth, recovery and healing.
Recognising the value/learning that can come from experiences of crisis. |
| Relational | Relationships are the basis of practice, and connection is used to build relationships of trust.
Recognises relationships built on trust and respect as foundational to working effectively with other Lived Experience workers and within multi-disciplinary environments. |
| Trauma-informed | Acknowledges the impact and prevalence of trauma, negative experiences and loss of control and power. Emphasises the need for physical, psychological and emotional safety. Creates opportunities for empowerment and for people to take an active role in their own healing/recovery. This is also captured in the lived experience conviction that it is better to ask “What happened to you?” not “What is wrong with you?” |
| Humanistic | The relational nature of Lived Experience work is recognised for its effectiveness to engage people through human connection and a holistic focus. |
| Voluntary | Participation is always voluntary (not coercive) and Lived Experience workers often take an active role in working towards eliminating forced treatment and restrictive practice. |
Personal and Family/Carer roles
Lived Experience roles have two distinct perspectives and ways of working and are informed by either:
- personal experience of mental health challenges, service use, periods of healing/personal recovery or
- experience of supporting someone through mental health challenges, service use, periods of healing/ personal recovery.
Most research into Lived Experience work has focused on personal or direct Lived Experience roles. There is little written about family/carer work and the similarities and differences between the roles. Building this knowledge base is key to supporting people in both roles to maintain the authenticity of their identified perspective.
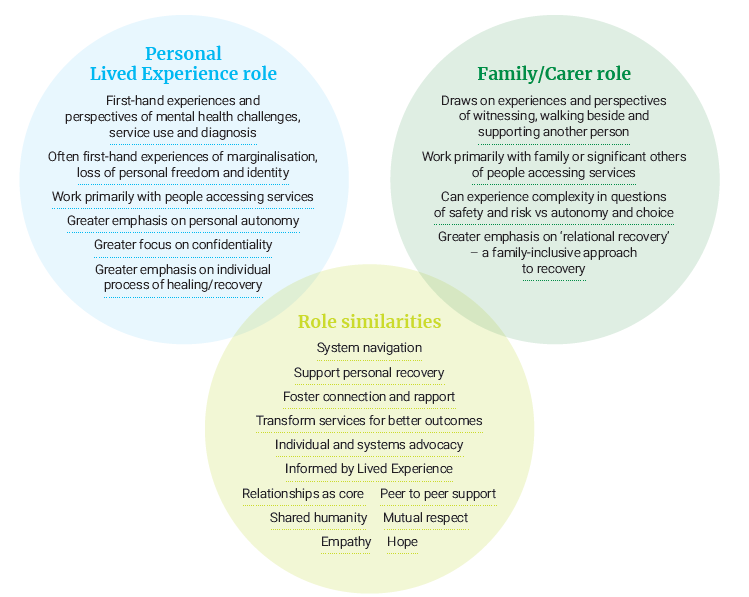
Similarities between personal Lived Experience and Family/Carer roles
Similarities between the roles centre on the values that underpin the work; differences relate to type of experiences, perspectives, and populations. Workers in both role types highlight the need for mutual respect and understanding, recognising the benefits of learning from each other and working collaboratively.
Both personal lived experience and family/carer roles stress the importance of hope, shared humanity, and empathy. Both roles share the goals of supporting personal recovery and transforming services to better meet people’s needs and both roles were considered to hold relationships as core to the work, both are also informed by lived experience.
Many skills are similar across personal lived experience and family/carer roles including:
- fostering connection and rapport
- peer to peer support
- system navigation
- individual advocacy
- advocacy to achieve system change.
Differences between personal Lived Experience and Family/Carer roles
Personal Lived Experience roles require first-hand or direct experience of service use/diagnosis/challenges and the consequent impacts. Whereas people in designated family/carer roles are employed to draw on their experience of having witnessed, walked beside and supported someone having those experiences. Ultimately, the roles differ in terms of who is being supported and whose perspective is primarily being represented (either the people accessing support or their family/carers/significant others). This results in differences in work practice.
While both aim to support personal recovery, family/carer workers may be more inclined to view recovery as a ‘relational’ rather than an ‘individual’ process: emphasising the importance of interpersonal relationships and a more family-inclusive approach to recovery. For people accessing services and those in personal Lived Experience roles, this focus may be less emphasised depending on an individual’s experiences with their family/significant others, broader consumer perspectives, and experiences of the impact of coercive treatment and discrimination (within systems, society and sometimes, families).
Depending on the individual’s experiences, people in the two role types may have different views about certain work practices. For example, personal Lived Experience workers are more likely to have a first-hand understanding of the traumatising impacts of coercive and involuntary practices. As a result, they are often more likely to emphasise the personal toll of human rights infringements. For some family/carer workers, concerns about safety and risk can make the question of coercion more complex.
Identified differences are also found in how values are applied within work practice. People in personal Lived Experience roles generally place greater emphasis on:
- upholding personal autonomy/respecting a person’s right to make choices and decisions
“nothing about us without us”
Further research is needed to improve the understanding of family/carer roles, including similarities and differences between family/carer roles and personal Lived Experience roles. This is a priority area for funding.
Figure 2: A comparison of personal and Family/Carer roles
Multiple types of experience
In reality, many people have experiences of both direct or first-hand service use/diagnosis/challenges, and experiences supporting others. Most people gravitate to the job type that reflects whatever experiences were most life-changing for them, i.e. made the most significant impact on their lives and sense of self. For some, this may change over the course of their lives, and some people are employed at different times in either personal lived experience or family/carer roles.
Roles that combine both personal Lived Experience and Family/Carer perspectives
Working in a role utilising both perspectives is likely to cause confusion, issues with boundaries, and conflicts of interest. Combined roles are not recommended and should not be considered without intensive exploration and consultation with the Lived Experience workforce and agreement reached by both personal (consumer) and family/carer leaders and workforces.
Family/carer workers can provide short-term, generalised support and referrals to people accessing services if this is welcomed by the individual. Similarly, people in personal Lived Experience roles may provide generalised support and information to family, carers or significant others.
Due to the mutuality of peer support and the emphasis on equal power, peer support relationships are seen to occur between people with ‘like’ experiences, (i.e. personal Lived Experience workers engaging in peer support relationships with people accessing services; family/carer workers with family, carers or significant others.) This is important to uphold lived experience values, particularly in situations where people accessing services have experienced family violence and/or trauma in the home.
It is recommended that job titles distinguish which perspective Lived Experience workers are working from to ensure transparency.
Specialisations
Specialisations build on the core skills of the Lived Experience workforce and contribute specific skill sets in areas of work and knowledge relevant to particular experiences, populations or settings. The development of Lived Experience specialisations mirrors what has occurred in other health and community service disciplines. Increasingly, designated Lived Experience workers, like non-designated workers, may be either generalists or specialists.
Although specialisations are still relatively new in the designated Lived Experience workforce, early indications suggest specialisations are valued as they acknowledge intersectionality and increase the relevance of support for people from diverse backgrounds and experiences. Intersectionality recognises that many people will have overlapping experiences, identifications and/or backgrounds that impact on, and influence their perspective and situation. Understanding how diverse experiences share commonalities and are related, is useful in Lived Experience work and enhances the effectiveness of specialisations.
Figure 3: Role specialisations

The growth of specialisations has brought a number of challenges. For example, current funding, structures and systems do not always support the employment of specialist Lived Experience workers. Developing the knowledge-base through research initiatives, and placing an emphasis on building the perceived value of diversity and inclusion will assist to address this.
As with all Lived Experience workforce development, the development of specialist roles and/or services must be led by Lived Experience leaders and workers who have those specific experiences, identifications or backgrounds. Specialist roles and services must also be guided by the existing knowledge and values of the wider movement and defined by an experience of both mental health challenge/supporting someone and the specialist area.
The National Development Guidelines companion document, ‘Lived Experience Roles: A practical guide to designing and developing Lived Experience positions’, provides additional information on specialisations. All Guidelines documents are available for download on the Commission’s page: https://www.mentalhealthcommission.gov.au/lived-experience/lived-experience-workforces
Lived Experience leadership
Lived Experience leaders are important to support the Lived Experience workforce and to ensure that decisions and practices are informed by lived experience at all levels. For people in Lived Experience ‘leadership’ or senior roles (including designated Lived Experience management, education, training, and research positions) it is strongly recommended they have worked previously in Lived Experience positions, and critical that they have understanding and can demonstrate connection to the broader consumer movement/Lived Experience workforce. Like any senior role, designated Lived Experience leadership roles are not an entry level position. Rather, they require deep understanding and ability to actualise the concepts and practices of Lived Experience work.
Allies/advocates of the Lived Experience workforce
Allies are essential to the success of designated Lived Experience workforce development. Allies are people employed in non-designated roles who actively champion and promote the Lived Experience workforce. The role of an ally is to support the Lived Experience worker to navigate the system, understand the business rules and ways of working so that they can better advocate for change. Allies recognise their position of privilege and accompanying responsibility in advocating for change to support the designated Lived Experience workforce. They vocally and practically support the designated Lived Experience workforce, are instrumental to social and organisational change and play a vital role in both the initial preparation and ongoing development of the designated Lived Experience workforce.
The term allyship is used to denote the ongoing process and role of allies. Allyship is needed at all levels within organisations, including colleagues, management, and funding bodies to ensure that understanding, acceptance and collaboration with Lived Experience workers is promoted and prioritised throughout the workforce. Allies who are independent or external to organisations also provide valuable additional support and advocacy. Allies may step into an advocacy position to support Lived Experience workers to self-advocate, advocate by publicly showing support for Lived Experience workers, or advocating for systemic changes. Allyship can be demonstrated at each level of the sector/individual organisations.
The issue of power is central to allyship and allies actively work towards equity and shared power with Lived Experience workers. They recognise and consciously work to remove barriers for the Lived Experience workforce, including practical constraints, attitudes/workplace culture, and bureaucratic processes that restrict effective Lived Experience work.
Broadly, effective allyship is recognised when allies engage in the following actions:
- actively oppose discriminatory language, policies and practice
- actively and vocally support the work of the Lived Experience workforce
- work collaboratively and respectfully in authentic partnerships
- defer to and step aside to credit lived expertise and share power
- facilitate opportunities for Lived Experience leadership
- seize opportunities to creatively use resources and invest in Lived Experience roles
- advocate for Lived Experience roles at multiple levels
- engage in co-production
- educate, organise and involve others in supporting the Lived Experience workforce.
Allies each have a range of skills; hence, multiple allies with different skills are necessary to enact change. Succession training is also essential so that the gains are not lost when allies leave the organisation. Training, co-developed by Lived Experience workers and experienced allies, can equip new allies to effectively take on the role of allyship.
A key area for action is to enlist and encourage allies in positions of authority who can advocate to progress Lived Experience workforce development. Succession training is required during staff turnovers to ensure that the work of allies continues.
Figure 4: Actions of allies in different roles
Colleagues
- ‘call out’ practices that violate values and principles of Lived Experience work and personal recovery
- educate other colleagues on the value and benefits of Lived Experience work
- recommend Lived Experience workers for roles
- advocate for Lived Experience leadership roles
- advocate for meaningful co-production
- create formal and informal networks, meetings and processes to increasingly involve more potential allies and Lived Experience workers
- guide new Lived Experience workers and share knowledge of navigating internal processes and organisational systems
- refer consumers and families to Lived Experience workers
Managers/governance
- demonstrate tangible commitment to workplace conditions and policies that support authentic Lived Experience work
- promote Lived Experience work to the whole workplace, people accessing services, their families and significant others
- build co-production as routine practice
- encourage collaboration and networking
- invest in professional development and career pathways to build Lived Experience leadership
- use resources creatively to increase Lived Experience roles
- allocate committed funds for Lived Experience workforce development
- take a proactive stand against discrimination and prejudicial attitudes
Funding bodies/policy makers
- investing substantially and sustainably in Lived Experience work
- require service delivery to incorporate Lived Experience roles
- ensure funding guidelines are informed by best practice e.g. more Lived Experience leadership
- ensure that the Lived Experience workforce is incorporated into new overarching policies and practices
- provide leadership roles for Lived Experience within funding bodies, including government bodies and commissioning bodies
- advocate and invest in stable and ongoing Lived Experience roles and Lived Experience-led programs
- make meaningful co-design and co-production a requirement of funding
- fund Lived Experience-led training, research and resource development
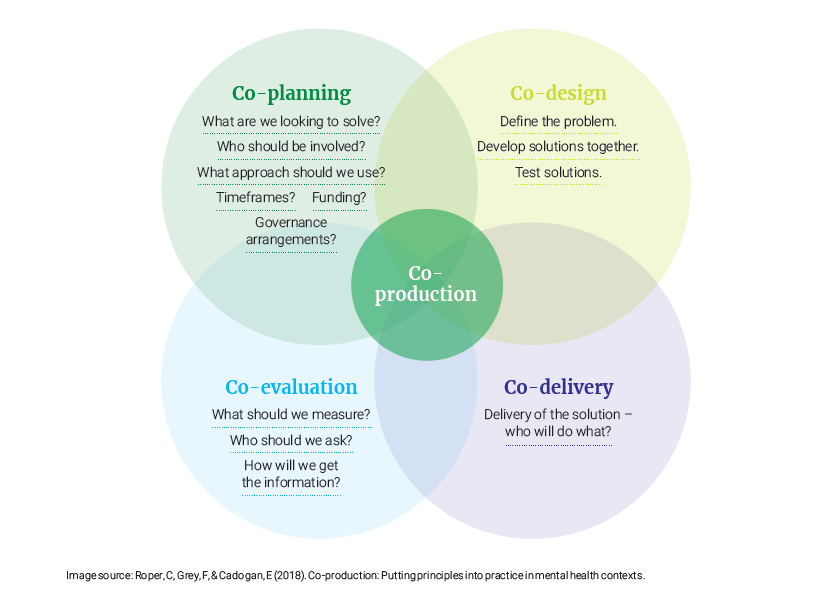
Co-production
Successful workforce development depends on the leadership and active engagement of people with lived experience and the communities they come from. Workforce development should always be contextualised to local needs, reflecting the diverse perspectives of lived experience.
Co-production is increasingly cited in policy and practice, but not always well understood. For Lived Experience workforce development to be effective, meaningful co-production is critical. Co-production requires giving equal status to lived experience knowledge and acknowledging lived expertise in recovery-orientation, being person-directed, and better understanding the experiences and views of people accessing services.
Lived Experience work is based on mutual sharing, with each person giving from their experience in a respectful exchange of knowledge as they contribute to problem solving. Like all other workers, Lived Experience workers are best able to contribute in an environment of equity, where there is fair and impartial inclusion.
Co-production requires equal partnership between designated Lived Experience and non-designated collaborators. True co-production means that designated Lived Experience workers need to be involved in providing meaningful input at all stages of development and review e.g. identifying the priorities to progress; and assisting in the planning, decision-making, design, delivery and evaluation of policies, practices, services, roles.
Co-production is effective when all parties feel valued and have the skills and confidence to contribute fully. For co-production to be transformational there must be a sharing of power between designated Lived Experience and non-designated workers. Proactive attention is needed to ensure designated Lived Experience collaborators are not inadvertently left out of the conversation or not having the jargon/language needed to participate fully.
Figure 5: Co-production
Co-production with Aboriginal and Torres Strait Islander communities
Australia’s First Nations Peoples represent two distinct cultures, Aboriginal, and Torres Strait Islander Peoples. Within these broad cultural groups there is also great diversity of cultures, languages, kinship structures and ways of life. Building strong understanding of Aboriginal and Torres Strait Islander perspectives and priorities for Lived Experience work and reform of mental health services is a vital part of the National Development Guidelines.
Service providers and funding bodies should have on-going conversations with Aboriginal and Torres Strait communities to explore what Lived Experience work involves, and how it might be viewed differently within communities, taking into account the need for acknowledging potential conflicts of workplace expectations versus the communities’ expectations, and concepts of social and emotional wellbeing.
Working with Aboriginal and Torres Strait Islander Peoples is complex and based within a history of colonisation, cultural practices, and protocols. It is therefore particularly important for organisations and funding bodies/policy makers to build relationships and gain guidance from Aboriginal and Torres Strait Islander sources locally, across jurisdictions, and nationally. It is vital that cultural governance be considered in all work with Aboriginal and Torres Strait Islander Peoples and carefully balanced against any implementation of clinical governance.
Lived experience recognises the effects of ongoing negative historical impacts and or specific events on the social and emotional wellbeing of Aboriginal and Torres Strait Islander peoples. It encompasses the cultural, spiritual, physical, emotional and mental wellbeing of the individual, family or community.
People with lived or living experience of suicide are those who have experienced suicidal thoughts, survived a suicide attempt, cared for someone through a suicidal crisis or been bereaved by suicide. It needs to be acknowledged that these experiences are significantly different and take into consideration Aboriginal and Torres Strait Islander Peoples ways of understanding social and emotional wellbeing.
‘The Aboriginal and Torres Strait Islander Lived Experience Centre’ is leading the creation of a culturally appropriate definition of lived experience, as well as a National Governance Group. This Centre will set up the support and structures required for culturally safe and informed Aboriginal and Torres Strait Islander lived experience voices. The Centre has been designed as a key contact for organisations and funding bodies/policy makers to build understanding and networks to ensure meaningful inclusion of Aboriginal and Torres Strait Islander perspectives and practices.
This aligns with the foundational principles of the Gayaa Dhuwi (Proud Spirit) Declaration and the definition of Lived Experience for Aboriginal and Torres Strait Islander communities published by the Black Dog Institute.