The Commission acknowledges Aboriginal and Torres Strait Islander peoples as the Traditional Custodians of the
lands and waters on which we live, work and learn.
Aboriginal and Torres Strait Islander peoples should be aware that this website contains images or names of people who have passed away
The National Children’s Mental Health and Wellbeing Strategy Report
Executive Summary
The National Children’s Mental Health and Wellbeing Strategy (the Strategy) provides a framework to guide critical investment in the mental health and wellbeing of children and families. There is nothing that will have more impact on improved mental health outcomes for all Australians than early intervention. Investing in the wellbeing of children and their families will have radiating benefits throughout our communities as well as through the broader health and education systems.
The Strategy provides clear pathways for proactively promoting child wellbeing and helping those who are struggling as early as possible to reduce long-term impacts of poor mental health. The Strategy adopts a broad scope to consider all settings in which children should be supported.
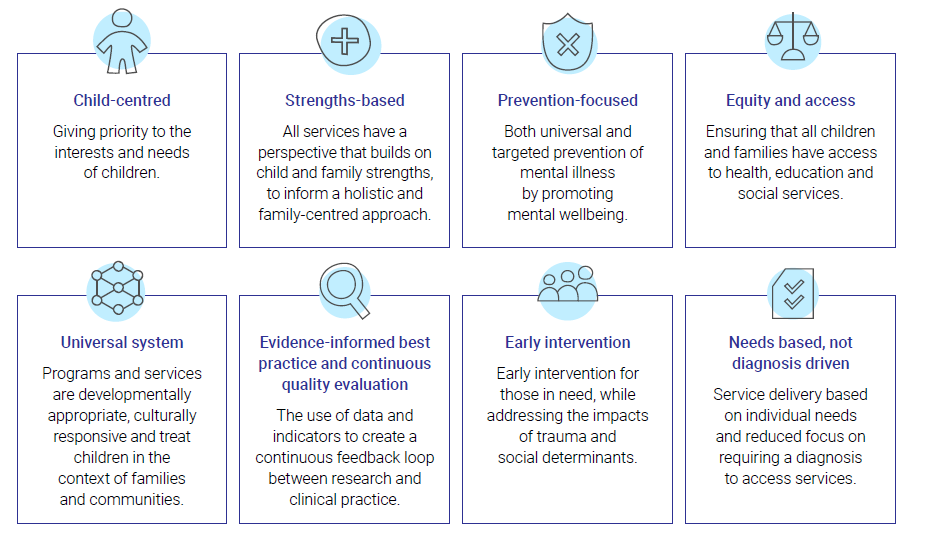
Eight principles have been used as the foundation of the Strategy’s development
These principles underlie the four focus areas of the Strategy.
Family and Community
The Service System
Education Settings
Evidence and Evaluation
Each focus area contains key objectives that need to be achieved, and each objective has multiple associated actions that are required to realise an optimal child mental health and wellbeing system.
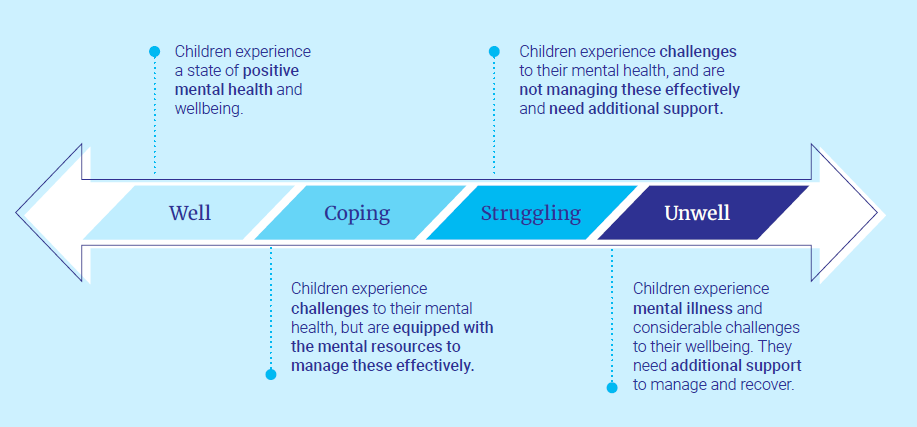
A wellbeing continuum
Importantly, beyond individual objectives and focus areas, the Strategy proposes a fundamental, cultural shift in the way we think about the mental health and wellbeing of children. This shift includes a change in language, adopting a continuumbased model of mental health and wellbeing. This moves away from terminology that may be stigmatising or too narrow to capture the full range of a child’s emotional experiences.
The continuum approach highlights that there are opportunities to promote improved wellbeing and possibly intervene before a child becomes unwell. It also focuses on a child’s functioning rather than diagnosis. For example, a child may have a diagnosed mental illness, but function well socially and educationally (i.e. ‘coping’). Similarly, a child who is ‘struggling’ might not require a diagnosis, but would be experiencing a decline in their usual functioning or anticipated developmental trajectory.
The optimal mental health system includes universal services and programs that help children remain in, or move to, the well end of the continuum. In addition, it would provide targeted supports and services for children who are struggling or unwell. The Strategy proposes that children should be able to access funded services at the point that they are beginning to struggle, rather than only once they are unwell and have received a diagnosis.
Consultations also found that this continuum approach aligns well with Aboriginal and Torres Strait Islander concepts of social and emotional wellbeing, which focus less on mental illness and more on holistic approaches to supporting wellbeing.
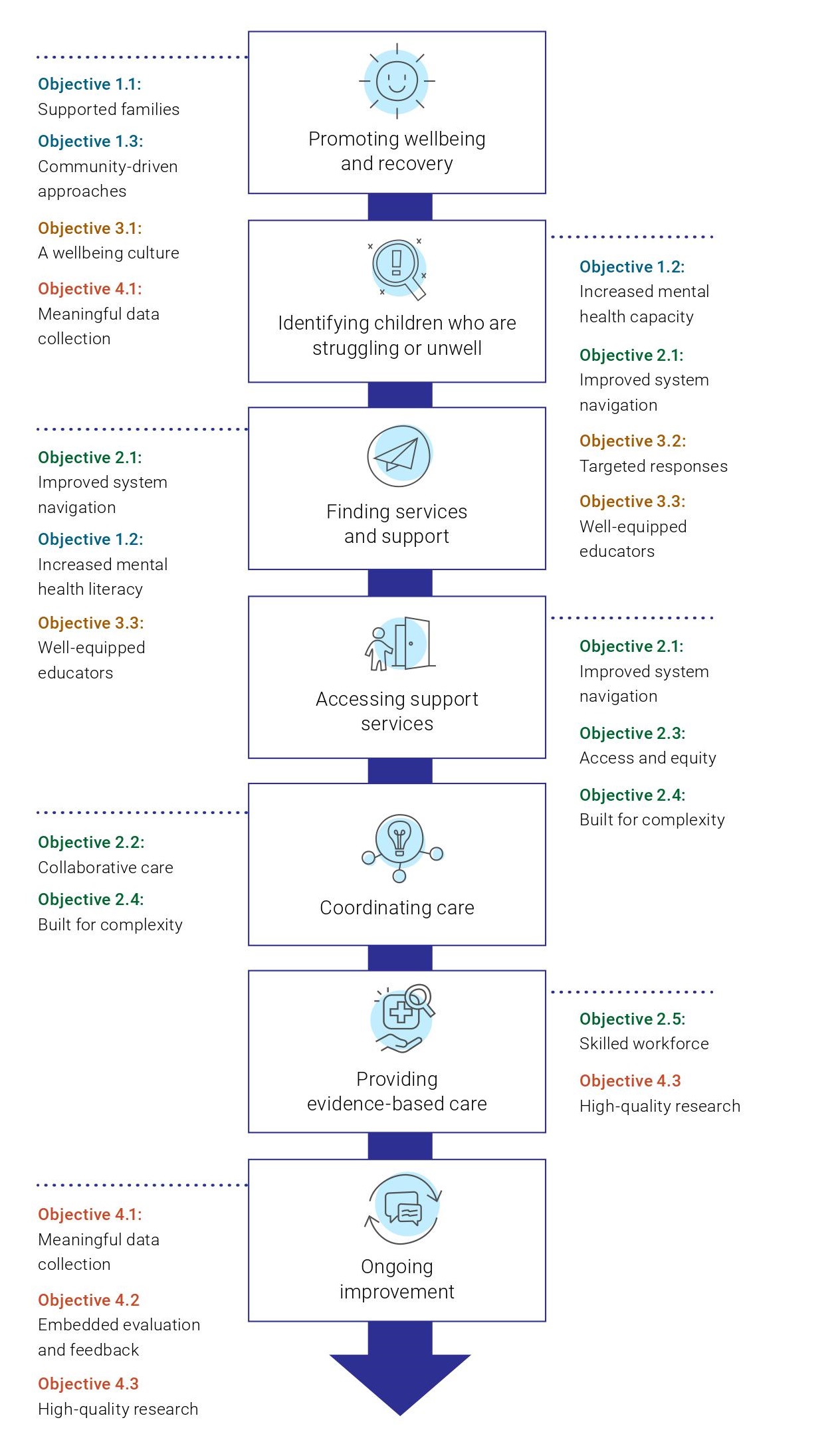
Objectives of the Strategy
The objectives in the Strategy collectively span all aspects of a child’s experiences of mental health, from promoting wellbeing and identifying children who are struggling through to providing evidence-based care and feedback and evaluation.
The figure on the right provides an overview of all objectives included in the Strategy. The objectives span across the focus areas and are numbered according to which focus area they align with, not in order of priority.
Family and Community
The Service System
Education Settings
Evidence and Evaluation
The following pages provide a snapshot of key content and priority actions across the four focus areas. These focus areas are equally important and their order in this Strategy does not imply priority or implementation sequence.
The focus area chapters provide additional depth beyond what is included in these snapshots. This includes existing approaches and tools we can build on, and indicators of change which may be used to monitor progress.
Focus Area 1: Family and Community
The Strategy highlights the importance of empowering families to promote mental health and wellbeing as part of routine parenting, and to actively collaborate with services when required. The importance of community-based approaches to health are also emphasised.
Objective 1.1 Supported families
Support for families should begin with addressing risk factors and challenges in the perinatal period.
Identifying parents who may be struggling is an effective strategy in promoting the wellbeing of their child.
Parenting programs should be promoted to all families at key developmental stages as a way of supporting child development.
Universal supports, such as parent helplines and antenatal courses, should be promoted and available in multiple languages.
Children not engaging with early childhood learning or primary school warrant systematic and proactive support.
Objective 1.2 Increased mental health literacy
Parents and carers may not recognise the signs of poor mental health in their child.
Signs that children are struggling can look different depending on developmental stage and may be impacted by culture and language background.
Increasing mental health literacy and reducing stigma must be supported by the whole community, and children must be supported to participate in conversations and decisions relating to their mental health.
Objective 1.3 Community-driven approaches
Social and geographical environments have significant impacts on mental health and wellbeing.
For children experiencing significant social and economic disadvantage, the needs of the broader community should be addressed to improve the mental health and wellbeing of the child.
Strong and supportive relationships both inside and outside the home can have a protective effect on mental health and wellbeing.
Priority actions
Increase parent and carer mental health literacy and their skills to support child mental health and wellbeing, via:
Routine offering of evidence-based parenting programs at key developmental milestones (action 1.1.c)
Emotional wellbeing modules embedded in antenatal and parenting courses (action 1.1.f)
Widely accessible evidence-based resources building on existing initiatives (action 1.1.b)
A national campaign promoting the value of parenting programs (action 1.1.d).
Support communities with the highest levels of need to address social and economic disadvantage (action 1.3.a) through:
Implementation of tailored programs focused on improving children’s mental health and wellbeing based on the key characteristics of successful place-based approaches (action 1.3.b).
Focus area 2: The Service System
The Strategy highlights the gaps in our mental health services, and how we can make it easier for children and their families to get help.
Objective 2.1 Improved system navigation
A lack of clear, consistent information about where to seek help delays access to services and creates additional stress and burden for families.
Existing navigational tools should be expanded to assist families to find local supports.
A model of integrated family care should be established and networked across Australia.
Consideration should be given to the transition between child and adult services.
Objective 2.2 Collaborative care
Collaborative care is a model that relies on multiple service providers and family communicating about what a child needs.
Increases in collaborative care approaches are required to ensure everyone understands what they need to do to support the child and family.
Objective 2.3 Access and equity
Many families are unable to access timely treatment, including due to high out-of-pocket costs, long waiting lists, dependency on diagnosis for treatment or high severity thresholds.
Resourcing, training and integration of face-to-face and telehealth approaches must be increased to improve access to supports.
Objective 2.4 Built for complexity
Children with complex needs are more likely to be turned away from support, as providers may not have the skills or resources required.
Priority access should be given to at-risk cohorts, including children in, or at-risk of entering, State care or in contact with the justice system.
Aboriginal Community Controlled Organisations should deliver supports for Aboriginal and Torres Strait Islander communities wherever possible.
Objective 2.5 Skilled workforce
Increased incentives for training in child and family mental health are required to encourage increased workforce participation, including in regional and remote areas.
Priority actions
Improve the capacity of systems to deal with complexity through:
Trialling (networked) sites in both urban and rural areas of a service model of integrated child and family care that exclusively provides holistic assessment and treatment for children 0-12 years old and their families (action 2.1.c)
Trialling sites with innovative service delivery models that integrate face-to-face and telehealth consultations, digital interventions, and phone helplines (action 2.3.c)
Providing support based on genuine co-design with children and families involved in the design, delivery and evaluation of services (action 2.3.e)
Allocating specific funding for care coordination for children and families with complex needs (action 2.4.a).
Requiring all government departments to outline and regularly report on what they do to support children in State care (action 2.4.d), including providing priority access to relevant services (action 2.4.c).
Amend current Medicare items to promote collaborative care including:
Enabling all providers (regardless of discipline) to claim for case conferencing (action 2.2.a)
Enabling providers to claim for consultations with parents and carers (without the child present) as part of the child’s care (action 2.2.c)
Requiring providers to communicate with educators and other service providers about a child’s treatment and support plan (action 2.2.d).
Focus area 3: Education Settings
The Strategy emphasises the important role that educational settings play in promoting mental health and wellbeing in children, and discusses the additional supports that may be required for educators to continue to build positive wellbeing cultures.
Objective 3.1 A wellbeing culture
There is currently wide variation between schools and early childhood learning services in the culture around mental health.
Some education settings have policies and procedures that contribute to stigma.
Introducing dedicated wellbeing staff and proactively promoting resources and support in education settings will assist educators to build positive wellbeing cultures.
Wellbeing programs should be included in early childhood curriculums and offered through after school and school holiday activities.
Objective 3.2 Targeted responses
All early childhood learning services and schools should have a wellbeing plan in place, tailored to meet the needs of their students.
Additional guidance is required to enable educators to discuss mental health concerns with parents and carers.
Proactive outreach procedures should be developed to respond to student disengagement, using trauma informed approaches.
Objective 3.3 Well-equipped educators
Professional training and clear guidelines and processes should be developed for educators to follow when they believe a child or family is struggling.
Dedicated wellbeing staff should establish and maintain strong relationships with local service providers such as paediatricians and psychologists, to promote collaborative care.
Educators should be supported to undertake additional learning on mental health, including with paid protected time for participation.
All educators should have access to avenues for support for their own mental health and wellbeing.
Priority actions
Ensure educators are well-equipped to support child mental health and wellbeing by:
Requiring all early childhood learning services and primary schools to have a comprehensive wellbeing plan for their students (action 3.2.a)
Providing funding to implement quality improvement activities and delivery of evidence-based programs targeting needs identified in wellbeing plans (action 3.2.b, 3.2.c)
Having a designated wellbeing staff member in all early childhood learning services and primary schools who is responsible for planning and co-ordinating wellbeing activities, including the development of wellbeing plans (action 3.1.b, 3.1.c).
Focus area 4: Evidence and Evaluation
The Strategy speaks to the importance of embedding a culture of evaluation in order to enable an optimal system of programs and services which provides consistently high-quality supports for children and families.
Objective 4.1 Meaningful data collection
Children’s mental health is an area where key population data are missing and there is currently no regular national data collection or reporting regarding children’s overall mental health and wellbeing.
A lack of data sovereignty means that programs or policies fail to reflect Aboriginal and Torres Strait Islander priorities, values, cultures, worldviews and diversity.
Increased and diversified data collection needs to be undertaken to inform delivery of programs and services.
Objective 4.2 Embedded evaluation and feedback
There is a growing number of clinical services and programs targeted at children’s and families' emotional wellbeing.
Only a small number of programs have robust evaluation embedded into program design. Service providers should be required to build evaluation into their programs.
Those using services have a valuable and essential perspective for informing service delivery.
Evaluations are most useful when they focus on the key outcomes that are important and meaningful to the children and families who have used a service.
Objective 4.3 High-quality research
Unlike youth mental health, there have been no national reforms or a framework for research focused on children in Australia. There is also an overall lack of community consultation and trials in child mental health.
Current ethics processes often make research with children challenging. Concerns around the vulnerability of children as a cohort could be better managed through including children and families in the development of research.
In the optimal system, children would receive measurement-based care with treatment improved based on ongoing feedback.
Priority actions
Ensure better collection and use of data through:
Establishing Inter-Departmental Committees to resolve current barriers to relevant data sharing across sectors such as education, justice and community health, for the purposes of informing child mental health and wellbeing (action 4.1.d).
Embedding evaluation in program and service delivery from the beginning, with reporting of findings required to receive further funding (action 4.2.a).
Including implementation evaluation as a core component of programs delivered in schools and early childhood learning settings to identify what is required to ensure fidelity (action 4.2.c).
Require supports to be based on and continue to involve high-quality research and evaluation through:
Funding parity for child mental health research and child physical health (action 4.3.a)
Targeted funding allocated on the basis of priorities including gaps in current treatment knowledge and the needs of priority populations (action 4.3.b).
Last updated:
Acknowledgement of Country
The Commission acknowledges Aboriginal and Torres Strait Islander peoples as the Traditional Custodians of the lands and waters on which we live, work and learn.
Diversity
The Commission is committed to embracing diversity and eliminating all forms of discrimination in the provision of health services. The Commission welcomes all people irrespective of ethnicity, lifestyle choice, faith, sexual orientation and gender identity.
Lived Experience
We acknowledge the individual and collective contributions of those with a lived and living experience of mental ill-health and suicide, and those who love, have loved and care for them. Each person’s journey is unique and a valued contribution to Australia’s commitment to mental health suicide prevention systems reform.